
Pharmacogenetics and hair loss treatments

Not all types of treatment work for everybody. This applies to all disease states, including hair loss.
The success of a given treatment to cure or prevent a disease depends on several factors. Namely a patient’s genetic profile and lifestyle.
Pharmacogenetics analyses how the genetic makeup of an individual affects his or her response to drugs and thinks beyond the culture of broad diagnosis that is commonly adopted by countries around the world.
Traditional treatment protocols, regardless of disease state, are symptom driven and assume a standard number of treatment types will be affective for all. The reality is this ‘one size fits all’ approach may only be effective for 30-60% of patients1.
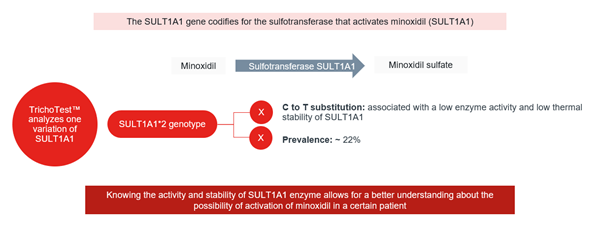
For hair loss, many patients apply a treatment containing minoxidil to the scalp. Studies indicate 22% of the global population will not respond positively to using minoxidil to treat hair loss2. So 1 in 5 patients using of minoxidil will not see any benefit or improvement.3-6
Furthermore, this will only become apparent after a patient applies the treatment for 6-12 months.
Pharmacogenetics provides opportunities to improve how we treat disease by delivering personalised treatments based on genomics and other clinical information. Personalised treatment is likely to improve a patient’s response, be more effective and reduce potential side effects.
Why is genomics important? As humans we are composed of cells and each cell contains a copy of our genes.
The study of these genes enables us to understand the genetic load inherited from our parents. Having this information allows us to decipher why we are unique, how our bodies function and our individual susceptibility to diseases such as hair loss.
Once we understand our genes, we can begin to understand how they may or may not react to pharmaceutical ingredients, such as minoxidil.
From a public health perspective, we can expect to see pharmacogenetics becoming more prevalent in the UK as the NHS focuses on genetic testing to improve patient outcomes. A number of initiatives are already underway such as the ‘100,000 Genomes Project’ that focusses on sequencing the whole genome of families with rare diseases and also other initiatives for patients with common cancers.
Genetic testing by way of simple DNA saliva samples are widely available to the public through private entities and online. Typically, they are used for uncovering information such as ancestry, nutrition and even the predictability of hair loss. In genomics terms these tests are low level and offer limited insight beyond potential yes/no outcomes.
More advanced genetic tests are becoming available for use by the general public in conjunction with healthcare professionals. One such test is Fagron TrichoTest™ which is a genetic test for hair loss that analyses gene variations and lifestyle factors.
Based on this information personalised hair loss treatments are recommended and informed treatment plans can be created by hair loss experts for patients.
The test analyses 48 genetic variations from a patient’s saliva sample. Detecting DNA variations, known as SNPs, facilitates the understanding of the specific characteristics of a patient’s metabolism that contribute to their hair loss.
The genetic variations analysed by Fagron TrichoTest™ are associated with 7 different categories of hair loss treatment: prostaglandins metabolism; inflammation; androgenic effect; vasodilation and blood circulation; collagen synthesis; vitamins and minerals metabolism; and insulin-like growth factor metabolism.
Understanding a patient’s genetic coding associated with these categories can help to identify how receptive a patient is likely to be to a particular pharmaceutical ingredient, such as minoxidil.
Results can be varied and are presented in a format which creates scope for the hair loss professional to allocate treatments and dosages accordingly.
Applying pharmacogenetics to hair loss in this way achieves a number of benefits for the patient.
Their treatment is personalised, according to their genes and lifestyle, and it is more likely to bring positive results.
They will be more invested in the process and the treatment regime and therefore compliance is likely to be far greater.
The likelihood of any treatments side effects will be reduced.
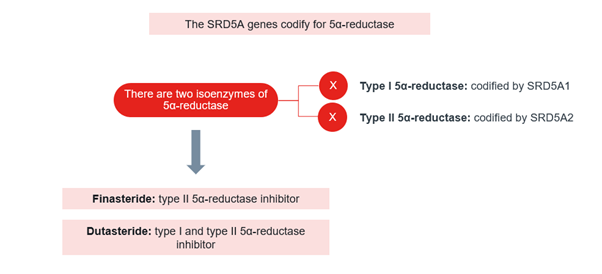
As an example, Finasteride, being one of the most used compounds to treat androgenetic alopecia, is also one of the drugs with higher prevalence of side effects, such as sexual disorders, swelling, dizziness, weakness, or skin problems. Finasteride also interacts with other drugs that the patient might be taking and therefore may increase the side effects risk. Dutasteride even though is a more modern drug it is also linked to similar side effects.
When TrichoTest analyses the genes related to the Finasteride or Dutasteride efficacy, one of the rationales behind is trying to avoid the usage of Finasteride or Dutasteride when it is not specifically required.
Therefore if TrichoTest determines that the SRD5A1 type I and type II isoenzymes are working normally, we will not recommend Finasteride/Dutasteride to the patient.7-12
With such algorithms we can avoid unnecessary side effects that, at the end of the day, reduce the patient adherence to the treatments.
Pharmacogenetics presents an enormous opportunity for trichologists, doctors and other professionals working with hair loss patients to improve patient outcomes via personalised treatment.
This is a sponsored blog by Fagron. The BAHRS has published this material for your information and does not actively endorse any products featured.

References:
1https://www.england.nhs.uk/wp-content/uploads/2016/09/improving-outcomes-personalised-medicine.pdf
2https://www.ensembl.org/Homo_sapiens/Variation/Population?db=core;r=16:28605693-28606693;v=rs1042028;vdb=variation;vf=22545139
3Buhl AE, et al. Minoxidil sulfate is the active metabolite that stimulates hair follicles. J Invest Dermatol. 1990 Nov;95(5):553-7.
4Goren A, et al. Novel enzymatic assay predicts minoxidil response in the treatment of androgenetic alopecia. Dermatologic Therapy, Vol. 27, 2014, 171–173.
5Raftogianis RB, et al. Phenol sulfotransferase pharmacogenetics in humans: association of common SULT1A1 alleles with TS PST phenotype. Biochem Biophys Res Commun. 1997 Oct 9;239(1):298-304.
6Grabinski JL, et al. Genotypic and allelic frequencies of SULT1A1 polymorphisms in women receiving adjuvant tamoxifen therapy. Breast Cancer Res Treat. 2006 Jan;95(1):13-6.
7Libecco JF, et al. Finasteride in the treatment of alopecia. Expert Opin Pharmacother. 2004 Apr;5(4):933-40.
8Hirshburg JM, et al. Adverse Effects and Safety of 5-alpha Reductase Inhibitors (Finasteride, Dutasteride): A Systematic Review. J Clin Aesthet Dermatol. 2016 Jul;9(7):56-62.
9Shiota M, et al. SRD5A gene polymorphism in Japanese men predicts prognosis of metastatic prostate cancer with androgen-deprivation therapy. Eur J Cancer. 2015 Sep;51(14):1962-9.
10Hsing AW, et al. Polymorphic markers in the SRD5A2 gene and prostate cancer risk: a population-based case-control study. Cancer Epidemiol Biomarkers Prev. 2001 Oct;10(10):1077-82.
11Allen NE, et al. The association between polymorphisms in the CYP17 and 5alpha-reductase (SRD5A2) genes and serum androgen concentrations in men. Cancer Epidemiol Biomarkers Prev. 2001 Mar;10(3):185-9.
12van Gils CH, et al. The V89L polymorphism in the 5-alpha-reductase type 2 gene and risk of breast cancer. Cancer Epidemiol Biomarkers Prev. 2003 Nov;12(11 Pt 1):1194-9.